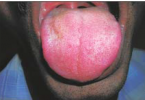
1. Pseudomembranous Candidosis
Clinical features
– White or creamy plaques that can be wiped off to leave a red base.
Incidence
– Rare in healthy patients.
Aetiology
– Neonatal or where oral microflora is disturbed by antibiotics, corticosteroids or xrostomia.
– Immune defects (especially HIV infection).
– Immunosuppressive management.
– Leukaemias and lymphomas,and diabetes.
Diagnosis
– Usually clinical, but Gram stain smear (hyphae) and blood picture may help.
– Differentiate from Koplik’s or Fordyce’s spots and lichen planus.
Management
– Treat predisposing cause.
– Antifungals : – nystatin oral suspension.
– Pastilles.
– Amphotericin lozenges.
– Miconazole gel or tablets.
– Fluconazole tablets.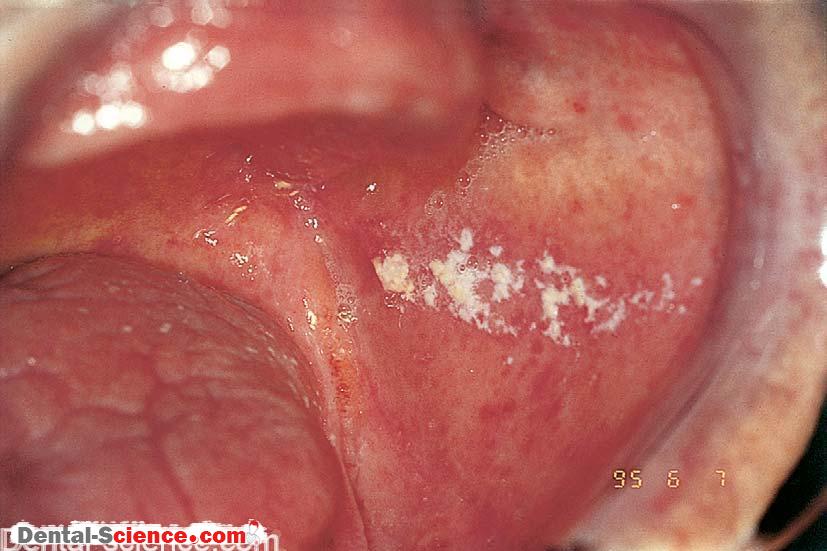


2. Erythematous Candidosis
– Candidosis may cause a sore red mouth, especially in patients on broad spectrum antimicrobials.
– Erythematous candidosis, especially on the palate or tongue, may also be a feature of HIV disease.

3. Chronic Mucocutaneous Candidosis
Clinical features
– Oral: persistent widespread leukoplakia.
– Cutaneous: nail and skin candidosis.
– Others: rarely familial multiple endocrinopathies.
Incidence
– Rare.
Aetiology
– Immune defects sometimes identified; occasionally genetic.
Diagnosis
– Family history, biopsy, blood picture, autoantibody and endocrine studies.
– Differentiate from other white lesions.
Management
– Antifungals.
4. Candidal Leukoplakia
Clinical features
– Candidal leukoplakia is typically found at commissures, often speckled.
– There is a higher premalignant potential than many leukoplakias.
Incidence
– Uncommon.
Aetiology
– Unclear aetiology: smoking predisposes.
Diagnosis
– Biopsy.
– Differentiate from other oral white lesions.
Management
– Antifungals.
– Smoking cessation.
– Removal (excision by laser or cryosurgery) or observation.